By Megan Jenkins | Trainee Midwife
It is a truth universally acknowledged that a country in possession of a high maternal and neonatal death rate, must be in want of more midwives. Indeed the World Health Organisation has declared that the best investment into healthcare services is in the midwifery workforce since midwives can provide 90% of the essential care needed for women and newborns and contribute towards ending preventable maternal and neonatal deaths. And yet in many countries women are still dying in childbirth as they have no access to midwives. In the remotest mountain regions of Myanmar (Burma) whole communities are born, live, give birth and die without the support of healthcare, hospitals, doctors or the much needed midwives. Instead these women rely on the bravery and courage of their fellow village women, their Traditional Birth Attendants (TBAs) to safely monitor them through pregnancy, support them to birth their babies and guide them through the fragile early days of motherhood helping them to nourish and sustain their babies. These TBAs provide a lifeline for the most desperate women, and yet many of them are illiterate, uneducated and have received no training. Knowledge, combined with cultural tradition, is passed down through the generations of TBAs and they learn their skills from village elders or their own mothers. Whilst their experience is huge, their knowledge and practice is not evidence based and can be unsafe.
In April 2018 I travelled out to Burma with 2 midwives to deliver a TBA training programme. Four days of travel navigating the almost impassable dramatic mountain passes of Chin State brought us to Lailenpi, a sprawling mountain village clinging to the dusty slopes, deep in the jungle and overlooking the border with India. A village little known to the outside world, and yet entirely alive with a vibrant Christian community.
Forty TBAs had gathered in Lailenpi. They had come from 12 different villages. Some of them arriving on the back of motorbikes, some of them walking for several days over the mountains, such was their eagerness to come and be trained by the ‘English midwives’.
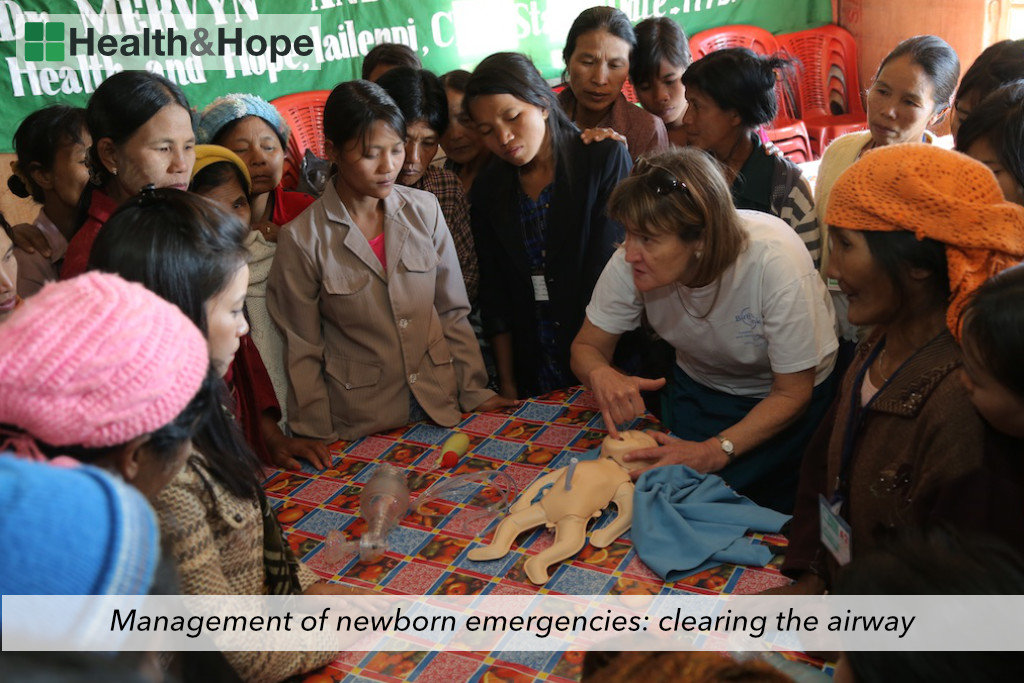
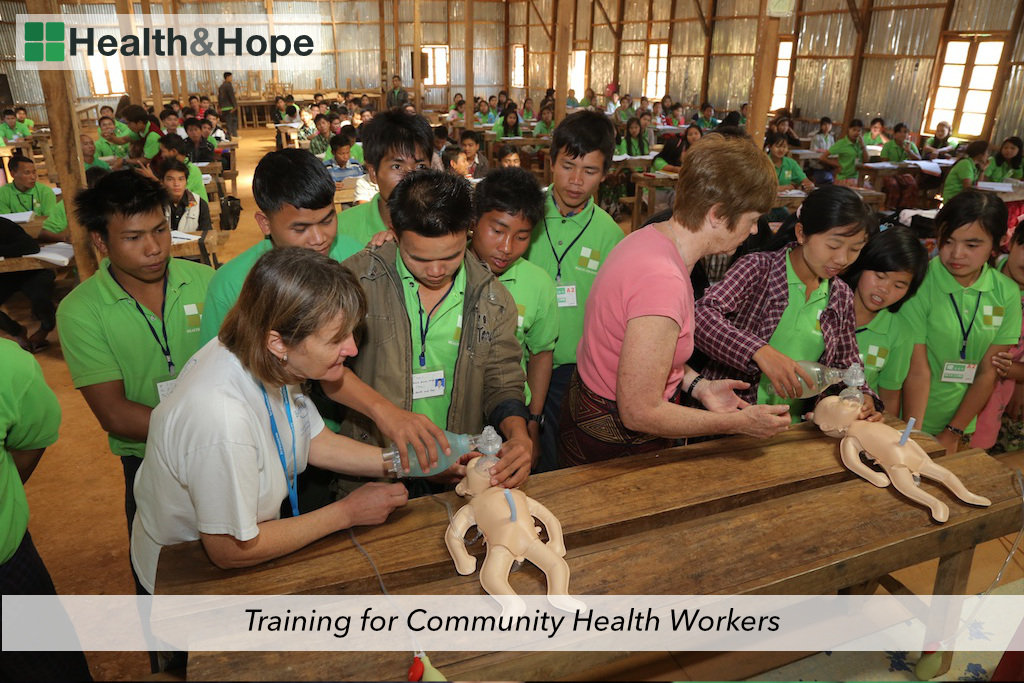
Over the 10 days we delivered a dynamic and interactive series of lessons from education on reproductive health, family planning, protection and prevention of sexually transmitted infections, antenatal health and care of the pregnant woman, postnatal care, recognising the unwell mother or baby and the importance of referral into the healthcare system. Teaching could be as simple as the importance of handwashing for the prevention of the spread of infection, or how to encourage and support upright, active birth to the complexities of managing obstetric emergencies of a shoulder dystocia, a postpartum haemorrhage and neonatal resuscitation. Each lesson was carefully chosen for its potential for impact. We were teaching the skills that transcend language barriers and are transferable across international borders.
As the week unfolded the team of disparate women formed a sisterhood, sharing their experiences of birth and death. Together we laughed and cried and as they saw our respect grow for their extraordinary wealth of experience so their trust in us grew and friendships formed. With mutual appreciation for one another the teaching and learning was powerful. These women are used to learning by rote, not to question, just to accept. By the end of the week they were all probing for answers in order to further understand the anatomy and physiology of birth mechanisms and how their actions could help to prevent morbidity and mortality. Watching the enlightenment on their faces as they grasped a new concept was the best reward we could ever ask for. One TBA said at the end of the training ‘Rote learning is what we have always done. These topics are so great because we can see, hear, touch and ask any questions we want to. The practical sessions are so helpful because you can really imagine and practice.’
What did we achieve? If the effects of this training reach no further than these 40 women, we know that there now exist 40 women empowered with knowledge and understanding, with skills of communication, team work and the realisation that their contribution to maternal and neonatal health is so greatly valued.
Yet we know that this training programme has much greater effect than individual empowerment. Since the TBA training programme launched in 2013 no mother in the town where the project was started has lost her life in childbirth, thanks to the skills that the TBAs have been equipped with. As such they have now closed the under 5’s section of the orphanage in Lailenpi. What greater testament could there be to the power of education, knowledge, midwifery skills and the contribution of TBAs, than the closing of an orphanage?
However, far greater than what we were able to give, was what we gained from living amongst these open and kind women. Received into their homes and lives we became engrained in their culture and traditions. Every night we were visited in our wooden house on stilts by a small group of TBAs bringing us gifts and offerings of eggs from their hens, bananas and papaya fruits, wild honey they had harvested from the jungle, small fish from the river and fabrics they had woven. These people of Chin State, who have very little themselves, were unendingly generous in sharing everything with us, from food to friendship, in order to show their gratitude for what we had come to teach them. The experience was humbling and inspiring and I can’t wait to return to them.
Links:
By Michelle James | Communications Officer
By Michelle James | Partnerships Executive
Project reports on GlobalGiving are posted directly to globalgiving.org by Project Leaders as they are completed, generally every 3-4 months. To protect the integrity of these documents, GlobalGiving does not alter them; therefore you may find some language or formatting issues.
If you donate to this project or have donated to this project, you can receive an email when this project posts a report. You can also subscribe for reports without donating.